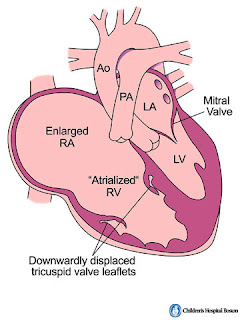
Ebstein's anomaly
risk of anomaly 1 in 20,000
higher frequency in mothers who take lithium
tricuspid valve leaflet
anterior leaflet - largest leaflet and attached to valve annulus, large, redundant
posterior and septal leaflet- vestigial/ absent - (failure of delamination of leaflets) when present the leaflets free edges are generally displaced posteriorly and downwards from AV junction and progressively towards the RVOT
RV
the RV i divided into two parts - proximal part - atrialized RV and distal part is RV proper and is small
Different classifications to describe Ebstein's -
type I--> IV (IV is the worst)
Associated cardiac defects -
ASD, PFO, VSD, PDA, RVOTO, Coarctation, WPW, LVNC
Differential diagnosis of Ebstein's
- tricuspid valve dysplasia
- tricuspid valve prolapse
- TV endocarditis
- carcinoid heart disease
- Uhl's anomaly
- ARVC
EKG findings
RAE, RVH, RBBB, pre-excitation
ECHO
- TV displacement >0.8cm/m^2 of BSA compared to position of mitral valve
- Great ormond street scoring/ GOSE
RA+atrialized RV/ functional RV+LA+LV, greater the ratio worse is the prognosis
MRI - TV anatomy and RV size and function.
Anticoagulation in an Ebstein;s patient
- h/o atrial fibrillation
- h/o paradoxical embolism
EP studies in Ebsein's patients with refractory arrhythmia showed
- 50% had single accessory pathway
- multiple accessory pathways in 29%
- almost all types (single / multiple pathways/ no pathway), chance of recurrence is 25%
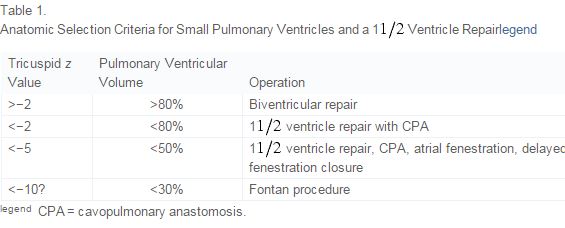
Indication for surgery
in infancy-
-severe cyanosis
- GOSE score with mild cyanosis
- CT ratio >80%
- severe TR
In older patients
- symptomatic
- exercise intolerance/
-cyanosis (sats>90%)
- paradoxical embolism
-progressive cardiomegaly
- progressive RV dilation/ deterioration in RV function

risk of anomaly 1 in 20,000
higher frequency in mothers who take lithium
tricuspid valve leaflet
anterior leaflet - largest leaflet and attached to valve annulus, large, redundant
posterior and septal leaflet- vestigial/ absent - (failure of delamination of leaflets) when present the leaflets free edges are generally displaced posteriorly and downwards from AV junction and progressively towards the RVOT
RV
the RV i divided into two parts - proximal part - atrialized RV and distal part is RV proper and is small
Different classifications to describe Ebstein's -
type I--> IV (IV is the worst)
Associated cardiac defects -
ASD, PFO, VSD, PDA, RVOTO, Coarctation, WPW, LVNC
Differential diagnosis of Ebstein's
- tricuspid valve dysplasia
- tricuspid valve prolapse
- TV endocarditis
- carcinoid heart disease
- Uhl's anomaly
- ARVC
EKG findings
RAE, RVH, RBBB, pre-excitation
ECHO
- TV displacement >0.8cm/m^2 of BSA compared to position of mitral valve
- Great ormond street scoring/ GOSE
RA+atrialized RV/ functional RV+LA+LV, greater the ratio worse is the prognosis
MRI - TV anatomy and RV size and function.
Anticoagulation in an Ebstein;s patient
- h/o atrial fibrillation
- h/o paradoxical embolism
EP studies in Ebsein's patients with refractory arrhythmia showed
- 50% had single accessory pathway
- multiple accessory pathways in 29%
- almost all types (single / multiple pathways/ no pathway), chance of recurrence is 25%
Indication for surgery
in infancy-
-severe cyanosis
- GOSE score with mild cyanosis
- CT ratio >80%
- severe TR
In older patients
- symptomatic
- exercise intolerance/
-cyanosis (sats>90%)
- paradoxical embolism
-progressive cardiomegaly
- progressive RV dilation/ deterioration in RV function

Comments
Post a Comment